
A surgeon’s thinking : An algorithm
Surgery is craftsmanship involving the application of manual dexterity with purpose. It is deliberate infliction of mechanical trauma and/or correction of effects of trauma to a consenting patient for the betterment of the patient. This blog, I hope, will encourage you to think deeply about how a surgeon (like me) approaches their work.
At the outset, I want to include a disclaimer. This blog does not offer medical recommendations and serves no therapeutic, diagnostic, or preventive purpose. Its sole aim is to share my personal views, which are not universally applicable.
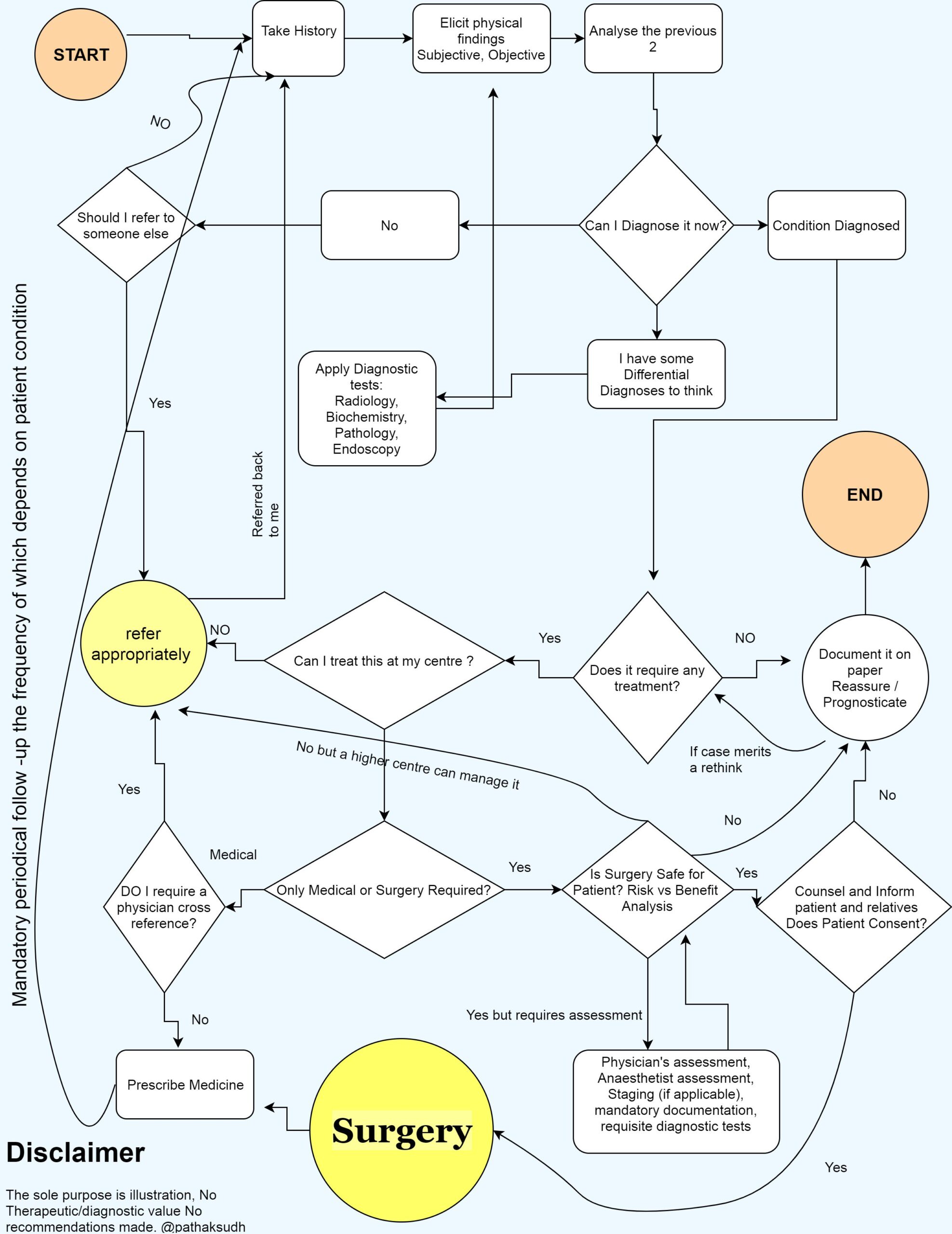
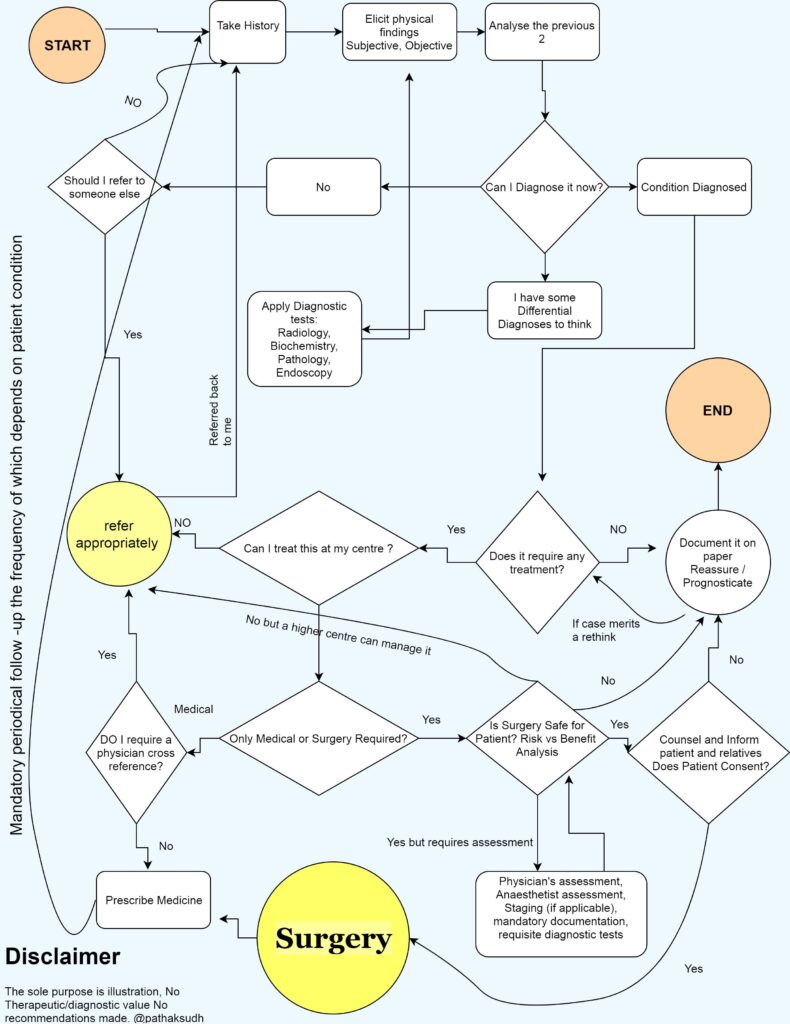
If you examine the algorithm (see diagram), you’ll notice it involves extensive decision-making and repetition.
One might think that collecting information is easy with standard checklists and questionnaires, and that’s true. Multiparameter monitors can automate the collection of objective data like pulse, blood pressure, and SpO2. However, collecting information is just one part of the algorithm. Many points require selection, where paths diverge. The first such point follows the history and physical examination. It takes considerable training to separate the essential from the irrelevant. I’ve noticed—and I’m sure every surgeon has—that this capacity is honed over years through repeated practice. And it continues to refine with each passing year.
Before a surgery is decided:
Before scheduling a patient for surgery, surgeons must establish a clear indication for the procedure. Fortunately, surgery’s role as a diagnostic tool has diminished over the past half-century. At the same time, the availability of high-quality diagnostic modalities has revolutionized the field. My generation of surgeons faces an abundance of imaging and investigative options, often involving multiple specialists. Precise and clear communication is critical at this stage. When surgeons clearly convey their clinical suspicions to radiologists or pathologists, it facilitates a precise diagnosis. This communication skill develops in proportion to the time a surgeon spends during residency and practice discussing CT scans, X-rays, and ultrasounds with colleagues, radiologists, and mentors. Similarly, surgeons must master the basic tenets of pathology to communicate effectively with pathologists.
Revealing a diagnosis to the patient is straightforward unless it involves cancer or a stigmatizing disease (a term I use reluctantly). In such cases, surgeons must involve close relatives and, if necessary, engage a trained counsellor.
Once surgeons establish a diagnosis, the next question is whether the patient requires surgery or any treatment at all. The answer lies in the well-known Latin phrase Primum non nocere, meaning “first, do no harm.” All surgeries, whether minor or major, carry some risk of complications, ranging from minor to life-threatening.
From our earliest training, surgeons learn to weigh the risks of surgery against its benefits and recommend surgery only when the benefits clearly outweigh the risks. This is easier to write than to practice. Surgeons draw inferences from peer-reviewed medical literature, learning from others’ experiences—both successes and failures—and understanding standard complications and their rates. We also rely on our own past experiences, maintaining logbooks and conducting surgical audits (topics beyond the scope of this blog). This process helps me determine whether my proposed surgery is reasonably safe (or, if risky, necessary to save a life). If the surgery is needed but my facility lacks the resources to perform it, I refer the patient to a higher centre.
Pre-anaesthesia Checkup
The next critical question is, “Is my patient safe for surgery?” The surgeon’s most trusted ally in the operating room, the anaesthetist, provides the answer. (A note of caution: in the UK, they are called anaesthetists; in the US, anesthesiologists. In India, it depends on personal preference—some dislike the term anaesthetist.) The anaesthesiologist conducts a pre-anaesthesia check-up, orders investigations for the patient’s safety, and sometimes requests consultations with a physician or cardiologist.
Once surgeons confirm the safety of the surgery for the patient and the patient’s fitness for surgery, they decide to proceed.
In the operation theatre:
Surgery is a serious endeavour, never to be taken lightly. We adhere strictly to Listerian principles of asepsis. It requires a team effort involving surgeons, anaesthesia team including consultants, nurses, and technicians. We use the WHO safety checklist to ensure we overlook no critical details, making the procedure as safe as possible for our patients. We prepare for any unforeseen incidents by reserving blood, administering antibiotics, keeping an emergency drug tray ready, and ensuring defibrillators are available.
Going into the technical nitty-gritties of surgery is beyond the scope of the present blog.
Care after the operation is over:
Post-surgery follow-up distinguishes us from mere craftsmen, transforming us into thoughtful practitioners. Surgeons follow a daily loop: eliciting history, assessing physical signs, ordering necessary investigations, and adjusting medical treatment until the patient no longer requires active intervention or can self-medicate. At that point, we discharge the patient with a reminder to follow up. In a minority of cases, complications arise, requiring us to repeat the same loop. If the necessary treatment is unavailable at our facility, we refer the patient appropriately.
Conclusions:
- Surgery is a serious endeavour.
- Surgical decision-making is a complex process, not always a linear sequence.
- It involves:
- Points of discretion and choosing one option over another, demanding experience, education, and adequate training.
- Multiple iterations of the same tasks, requiring devotion and dedication.
- A craft often practiced as part of a team with other doctors and paramedical staff.
- Referring a patient to a higher centre is neither a shrugging off of responsibility nor a mark of incompetence; it is often a wise decision for the patient’s benefit.
- Becoming a surgeon has no shortcuts: six years of pre-residency scientific training in the form of MBBS course and the internship, three years of gruelling residency to master surgical methods and skills, and many years of ongoing maturation.
Dr. Sudhanwa R. Pathak
MS, FAIS, FIAGES, DNB (GI Surgery)
Miraj, India
January 10, 2018
Edited: 10th June 2025
Great work Dr Sudhanwa. Nicely put.
Sudhanwa you are a good writer..Keep it up..
Vallabh
Very well written n precise.
Wonderfully written.
Mind blowing stuff
Nicely written in a very apt way
Sudhan, nicely written. Congratulations for the blog .